
Volume 39, Issue 1 ⦁ Pages: 5-15
Abstract
Binge drinking, commonly defined as consuming five or more standard drinks per occasion for men and four or more drinks for women, typically begins in adolescence. Adolescents, although they may drink less often, tend to consume higher quantities of alcohol per occasion compared with adults. This developmental difference in pattern of alcohol consumption may result, in part, from maturational changes that involve an adolescent-specific sensitivity to certain alcohol effects and greater propensity for risk-taking behaviors, such as binge drinking. Adolescent binge drinking is associated with a range of acute alcohol-related harms, some of which may persist into adulthood. The prevalence of binge drinking, including high-intensity drinking (i.e., 10 or more and 15 or more drinks per occasion), has declined among adolescents in recent years. Overall, however, the proportion of youth who engage in binge drinking remains high. This article reviews the definition and prevalence of binge drinking in adolescence, trajectories of binge drinking and their correlates, and implications for prevention.
Compared with adults, adolescent drinkers tend to consume higher quantities of alcohol per occasion but drink less frequently.1 Thus, underage drinkers ages 12 to 20 typically consume 4 to 5 drinks per drinking episode, which is nearly double the average of the 2 to 3 drinks usually consumed by adults (older than age 25).1 Most of the alcohol consumption of underage drinkers occurs during “binge” episodes characterized by drinking high quantities.2,3 This binge pattern of consumption has been linked to serious alcohol-related harm, such as alcohol poisoning, as well as to sometimes fatal injuries and accidents resulting from acute intoxication.4 The adverse consequences of adolescent binge drinking affect not only the adolescents but also their families, peers, and community.5
This article reviews various definitions of binge drinking, the acute adverse consequences associated with binge drinking, the prevalence of adolescent binge drinking, and demographic factors (e.g., gender and race/ethnicity) associated with adolescent binge drinking, and demographic factors (e.g., gender and race/ethnicity) associated with adolescent binge drinking. It then discusses the developmental context of adolescent binge drinking, including adolescent-specific sensitivity to certain alcohol effects that may contribute to episodes of high-volume alcohol consumption in adolescence. After a summary of trajectories of binge drinking in adolescence, trajectory correlates representing risk factors and young-adult outcomes, and possible neurocognitive consequences of adolescent binge drinking, the implications of research on adolescent binge drinking for prevention efforts are briefly reviewed.
Definitions of Binge Drinking for Youth
Binge drinking, or an episode of high-volume alcohol consumption, has been defined in various ways.6,7 (For more information, see Drinking Patterns and Their Definitions in this issue.) According to the National Institute on Alcohol Abuse and Alcoholism (NIAAA),8 “binge drinking” refers to alcohol consumption that brings the blood alcohol concentration (BAC) to .08 g/dL, which is commonly associated with acute impairment in motor coordination and cognitive functioning.9 BACs of more than .08 g/dL typically occur in men after consuming five or more drinks in about 2 hours, and in women after consuming four or more drinks. This is known as the “5+/4+” binge definition. This definition is consistent with epidemiological data indicating an association at the population level between greater frequency of 5+/4+ binge episodes and more adverse drinking-related consequences.10
When applied to adolescents, binge-drinking definitions based on adult levels of alcohol intake (e.g., 5+/4+ drinks per occasion) often are too high. Children and adolescents are likely to reach BACs of more than .08 g/dL at lower levels of consumption due, in part, to factors such as smaller body size. Donovan used an updated Widmark equation and population data on average body weight in boys and girls to estimate the levels of drinking that would produce BACs of more than .08 g/dL in youth ages 9 to 17.11 For those ages 9 to 13, a binge episode was estimated to occur with intake of 3 or more drinks within a 2-hour period; for those ages 14 to 15, with 4 or more drinks for boys and 3 or more drinks for girls; and for those ages 16 to 17, with 5 or more drinks for boys and 3 or more drinks for girls. These proposed binge-drinking thresholds for youth are theoretical and based on estimated, rather than observed, BACs. Nevertheless, the identification of lower drinking-quantity thresholds to define binge drinking for younger drinkers suggests that the use of standard adult-based binge definitions may underestimate the prevalence of drinking behavior that leads to BACs of more than .08 g/dL, particularly among females and youth.
Extreme binge, or high-intensity, drinking involves the intake of dangerously high quantities of alcohol per occasion. (For more information, see High-Intensity Drinking in this issue.) Thresholds of 10 or more drinks (i.e., double the usual definition of binge drinking of 5 or more drinks) and 15 or more drinks per occasion (i.e., triple the usual definition of binge drinking of 5 or more drinks), as well as gender-specific cutoffs of 8 or more drinks for females and 10 or more drinks for males, respectively, have been used to define high-intensity drinking.12-14 These definitions specify thresholds that are two to three times higher than the 5+/4+ binge definition and have been examined in part because of limitations in the reliability of the 5+/4+ binge definition for identifying drinkers with BACs of more than .08 g/dL.15 As a point of reference, among adolescent drinkers, alcohol-related blackouts, or acute alcohol-related memory loss, may occur after consuming nine or more drinks per occasion for males and five or more drinks for females.16
Acute Adverse Consequences of Binge Drinking
Acute negative alcohol-related consequences generally show a dose-response relationship with binge drinking,17 such that greater risk for many adverse consequences has been associated with higher drinking quantities and more frequent binge episodes.18-20 A significant literature has examined the diverse acute health harms associated with binge drinking, such as alcohol poisoning, alcohol-related blackouts and injury, involvement in car crashes and fatalities, alcohol-related physical and sexual assault, increased risk for sexually transmitted infection, and problems at school or work.4,21 Risk behaviors associated with binge drinking may include, for example, simultaneous use of other substances (e.g., marijuana) and greater likelihood of riding with an intoxicated driver.22 Although many of the acute adverse consequences of binge drinking are not unique to adolescents, young drinkers may be at higher risk than adult drinkers for certain acute alcohol-related harms (e.g., alcohol poisoning) because of their relative inexperience with alcohol’s effects. Importantly, although some adolescent heavy drinkers meet the criteria for an alcohol use disorder (2.7% of those ages 12 to 17), many more youth report binge alcohol use (6.1%)23 and may experience acute adverse effects from binge drinking that are not covered by diagnostic criteria.
Prevalence of Adolescent Binge Drinking
Numerous studies have assessed the prevalence of adolescent binge drinking in the United States, as well as in other countries. These studies also have assessed the association between binge-drinking rates and demographic characteristics.
Trends in the Prevalence of Adolescent Binge Drinking in the United States
Three national surveys in the United States provide data on the prevalence of adolescent binge drinking, including the National Survey on Drug Use and Health (NSDUH), which until 2015 defined binge drinking as consumption of five or more drinks on the same occasion;* the Monitoring the Future (MTF) survey, which defines it as five or more drinks in a row; and the Youth Risk Behavior Survey (YRBS), which defines it as five or more drinks of alcohol in a row—that is, within a couple of hours. (For more information on these surveys, see Surveys That Include Information Relevant to Binge Drinking in this issue.) Thus, until 2015, these surveys all used the same threshold to define binge drinking in males and females, albeit with slightly different wording and with differences in the time frame used to assess binge drinking (i.e., within the past month for the NSDUH and YRBS, and within the past 2 weeks for the MTF). The NSDUH has collected annual data since 1991 on individuals ages 12 and older using interviews conducted in the home.5 In contrast, both MTF and YRBS are school-based surveys. MTF has collected annual data since 1975 from 12th graders, and since 1991 from 8th, 10th, and 12th graders.24 YRBS has collected data biennially since 1991 from 9th to 12th graders.25
*Since 2015, the NSDUH defines binge drinking as consumption of 4 or more drinks for women or 5 or more drinks for men on the same occasion on at least 1 day in the past 30 days.
All three surveys show similar time trends in adolescent binge drinking.26 The MTF data indicate a peak in the prevalence of youth binge drinking in the late 1970s to early 1980s, followed by a decrease from 41% in 1983 to 28% in 1992.24 In the 2015 MTF survey, binge drinking in the past 2 weeks was reported by 4.6% of 8th graders, 10.9% of 10th graders, and 17.2% of 12th graders.24 This reduction in youth binge-drinking prevalence over time may reflect factors such as enactment of a minimum legal drinking age of 21 and other alcohol regulatory policies.4,27 Time-trend data from the YRBS (from 1999 to 2013) and NSDUH (from 2002 to 2014) indicate a similar decrease in youth binge drinking in recent years.5,25
The prevalence of high-intensity drinking (10 or more or 15 or more drinks in a row in the past 2 weeks) was relatively stable among high school seniors in the MTF from 2006 to 2012, but, like binge drinking, has shown a decline in recent years. Thus, the prevalence of consuming 10 or more drinks in a row declined from 10.4% in 2012 to 6.1% in 2015, and the prevalence of consuming 15 or more drinks in a row declined from 5.5% in 2012 to 3.5% in 2015.24
In all three national surveys, binge-drinking prevalence increases with age during adolescence. For example, in 2015, the most recent year in which all three national surveys collected data on binge drinking, NSDUH indicated that 9.6% of youth ages 12 to 17 reported alcohol use in the past month, with roughly half (i.e., 5.8%) of these drinkers reporting binge drinking in the past month.28 Among respondents ages 12 to 17 in the 2015 NSDUH, past-month binge-drinking prevalence increased from 0.5% at ages 12 to 13 to 15.3% at age 17. In the 2015 YRBS, 17.7% of all high school students reported binge drinking in the past month, increasing from 10.4% in 9th graders to 24.6% in 12th graders.29 According to the 2015 MTF survey, 4.6% of 8th graders, 10.9% of 10th graders, and 17.2% of 12th graders reported binge drinking in the 2 weeks prior to the survey.24
The results from these three national surveys are broadly consistent in a given year, although YRBS data generally indicate somewhat higher binge prevalences compared with NSDUH and MTF, and MTF tends to report higher prevalences compared with NSDUH.26 The differences in binge-drinking prevalence across the surveys may result from methodological differences, such as sampling strategy used, survey location (e.g., school or home), type of data collection (e.g., paper survey or self-administered computer assessment), item wording, and time frames for querying binge drinking.26 Interpretation of results from these national surveys also needs to consider that use of the “5+” binge definition in these surveys may underestimate the prevalence of binge drinking in younger adolescents and females, because, as mentioned earlier, lower drinking-quantity thresholds to define binge drinking are indicated in this age group.11
International Surveys of Adolescent Binge-Drinking Prevalence
International data on the prevalence of adolescent binge drinking are available from sources such as the European School Survey Project on Alcohol and Other Drugs (ESPAD) and the Australian School Students Alcohol and Drug (ASSAD) survey. In 2011, the ESPAD report on 15- to 16-year-old students in 36 European countries indicated that the average prevalence of consuming 5 or more drinks on at least 1 occasion in the past 30 days was 39% across countries.30 However, ESPAD countries differed in the average alcohol quantity that students reported consuming on their most recent drinking day. Thus, students in Nordic countries and the British Isles generally reported consuming a higher average quantity than did students in southeastern Europe (e.g., Greece or Italy).30 By comparison, the 2011 ASSAD survey found that among students ages 12 to 17 who reported drinking in the week prior to the survey (17.5% of all students queried), more than one-third (36.2%) drank 5 or more drinks in a day.31
In general, countries with lower legal drinking ages have a higher prevalence of adolescent binge drinking compared with countries with higher legal drinking ages.32 Also, rates of adolescent binge drinking generally are higher in many European countries4 and Australia31 than in the United States. However, such variations in binge-drinking prevalence across studies need to be interpreted with caution because methodological differences (e.g., in sampling method, ages covered, item wording, time frames, and the definition of a standard drink) exist across surveys.
Adolescent Binge-Drinking Prevalence by Demographic Characteristics
In general, males tend to report higher rates of binge drinking in adolescence than do females (see Figure 1).13,14,23,24 These gender differences typically increase with age during adolescence.22,30,33 However, time-trend data from MTF have indicated a narrowing of the gender gap starting in the mid-1970s, particularly among high school seniors. Thus, in the 1975 MTF, 49% of male high school seniors, but only 26% of females, reported binge drinking, corresponding to a 23-percentage-point difference. By 2014, in contrast, a mere 5-percentage-point difference existed between male (22%) and female (17%) high school seniors who reported binge drinking.33 Conversely, NSDUH time-trend data from 2002 to 2012 for youth ages 12 to 17 indicate that although binge drinking decreased for both males (from 11.3% in 2002 to 7.4% in 2012) and females (from 10.2% in 2002 to 6.8% in 2012), with more males than females reporting binge drinking at both time points, there was little support for a narrowing of the gender gap over these years.34 The time-trend results for gender differences from the MTF and NSDUH surveys are not directly comparable because of differences in the ages covered, as well as in item wording and time frames assessed (i.e., the MTF asked about 5 or more drinks in a row in the past 2 weeks, whereas the NSDUH asked about 5 or more drinks on an occasion in the past month). Nevertheless, both surveys indicate greater binge-drinking prevalence among male than among female adolescents.22
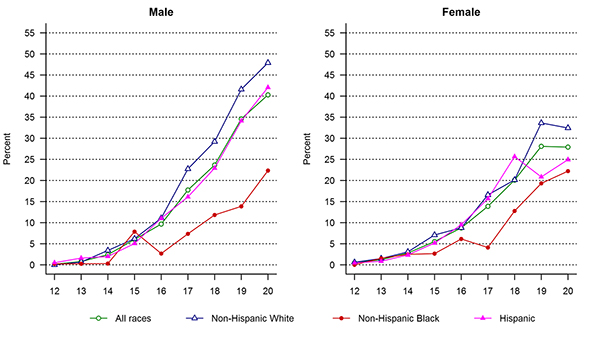
The prevalence of adolescent binge drinking in the United States also differs by race/ethnicity (see Figure 1). Among adolescents ages 12 to 17 in the 2014 NSDUH, the prevalence of past-month binge drinking was higher among Whites (7.1%) and Hispanics/Latinos (6.3%) compared with Blacks (3.6%) and Asians (1.5%).23 MTF time-trend data from 1975 to 2014 suggest that these race/ethnic differences may differ by year in high school.33 For example, among 8th-grade students, more Hispanics tended to report binge drinking compared with Whites and Blacks. Among 10th- and 12th-grade students, however, Hispanics and Whites were more likely to report binge drinking than were Blacks.
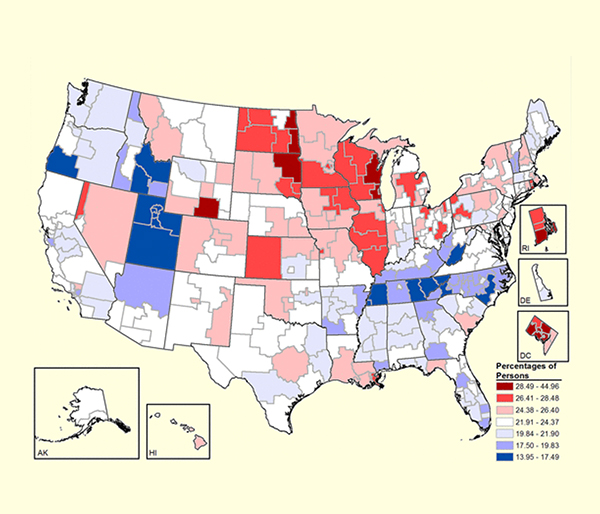
In the United States, binge-drinking prevalence also varies by region, with differences observed between and within states (see Figure 2).33 For example, based on recent NSDUH data, past-month binge-drinking prevalence among underage drinkers ages 12 to 20 at the state level was highest in four states in the Northeast, four states in the Midwest, the District of Columbia, and one state in the West.35 Even within a region, such as the District of Columbia, subregions differed in the prevalence of past-month binge drinking, ranging from 10.8% to 42.4% in the District of Columbia, with an overall estimate of 18.0%.35 High-intensity or extreme binge-drinking prevalence was especially high among high school seniors in the Midwest.13 Binge-drinking prevalence also differed by urban versus rural setting, with high school students living in rural areas tending to report the highest rates of binge drinking.33 These regional differences suggest that factors such as local and regional norms regarding alcohol use, as well as local alcohol regulatory policies and enforcement, have an important influence on prevalence of binge drinking.
Developmental Context of Adolescent Binge Drinking
During adolescence, ongoing brain development and rapid changes in physical maturation occur in the context of a shift from parents and family to peers as a primary source of support and guidance.36,37 These normative, adolescent-specific changes in physical maturation and social context can contribute to the risk for binge drinking. In particular, the fine tuning of the neural circuitry that occurs during this developmental period is associated with an adolescent-specific elevation in the ability to consume alcohol, which appears to be conserved across species.38 Animal (e.g., rodent) models indicate that neural changes occurring in adolescence may temporarily increase sensitivity to certain alcohol effects (e.g., rewarding effects) that promote consumption within a drinking episode, while reducing sensitivity to other effects (e.g., sedative effects) that may help to limit drinking during an episode.38 Evidence for such an adolescent-specific sensitivity to alcohol effects in humans is sparse but aligns with animal models to suggest that compared with their adult counterparts, human adolescents may be more sensitive to alcohol’s rewarding and stimulant effects39 and less sensitive to its sedative effects.40 Related research has found that, among college students, high-intensity binge drinking (i.e., 8 or more/10 or more drinks for females/males) is experienced as more rewarding than non–high-intensity drinking (i.e., less than 8/10 drinks for females/males).41 Furthermore, many college students reported willingness to tolerate adverse alcohol effects in order to experience the positive effects associated with high-intensity drinking.41
The adolescent-specific shift from family to peers as important sources of influence on youth attitudes and behavior also can contribute to risk-taking behaviors, such as binge drinking.42,43 Higher levels of sensation seeking and impulsivity, which are associated with risk-taking behaviors and binge drinking, tend to be endorsed more often by adolescent males than by females, which may help explain the generally greater prevalence of binge drinking among males.44 Risk-taking behavior may be facilitated by the presence of peers.43 Consistent with this observation, adolescent binge drinking tends to occur in social contexts with peers.45,46 This may encourage episodes of high-volume consumption through mechanisms such as peers providing access to alcohol, peer norms that are favorable to binge-drinking behavior, and positive feelings generated by social activities that involve alcohol use.37,47
Binge drinking among underage drinkers in the United States often involves distilled spirits, with consumption of beer reported in less than one-third of binge episodes.48 For some youth, consumption of liquor may reflect the intent to drink to get drunk as quickly as possible. The preferential consumption of liquor by adolescents during binge episodes is particularly concerning because it has been linked with increased risk for alcohol-related consequences, such as blackouts or injury.49
Young drinkers also often lack knowledge regarding standard drink servings, particularly for spirits, which can result in overpouring—that is, pouring greater volumes than used for standard drink servings.50 Overpouring can increase the likelihood of high-volume consumption, rapid intoxication, and risk for certain alcohol-related harms, such as blackouts.50
Other contextual factors relevant to adolescent binge drinking include the places where drinking occurs and the temporal patterning (e.g., weekend or seasonal) of drinking. For example, certain places where adolescent binge drinking occurs, such as at someone else’s home without parental supervision or at a bar or nightclub, have been associated with greater risk for alcohol-related violence.51 With regard to temporal patterning, the timing of adolescent binge drinking shows some predictability: Binge drinking may be more likely to occur during weekends, summer and spring breaks, holidays (e.g., New Year’s Eve), and occasions such as prom and sports events.52 These contextual factors, in combination with an adolescent-specific sensitivity pattern to alcohol effects and the peer social context of drinking, may interact with individual difference factors, such as heritable risk and exposure to trauma, in contributing to increased risk for binge drinking and related harm in adolescence.38
Binge-Drinking Trajectories in Adolescence
The onset of alcohol use peaks during grades 7 to 11.24 By 8th grade, 11% of students report having been drunk (a self-report proxy for high-quantity consumption) at least once in their lifetime, with an increase to 29% among 10th graders and 47% among high school seniors.24 Reports of the onset of consuming 3 or more drinks per occasion begin to increase between ages 13.5 and 15.5, and reports of an episode of binge drinking (5 or more drinks per occasion) start to rise around age 16.53 Although rates of binge drinking peak between ages 18 and 25,54 the onset of binge drinking (i.e., 3 or more or 5 or more drinks per occasion) and episodes of being drunk typically occur in early to mid-adolescence (i.e., ages 12 to 16). Early age of first intoxication (younger than 15 years old) and rapid progression from first drink to first intoxication both are early warning signs of heavy, particularly binge, drinking.55,56
Longitudinal studies that span adolescence through emerging adulthood (i.e., ages 12 to 25) have identified three to five prototypical trajectories of binge drinking (see Figure 3).57-63 The trajectories derived in these studies provide useful heuristics for under-standing different patterns of change in binge drinking across adolescence. They highlight heterogeneity in course, and differ with respect to age at onset of binge drinking; timing, rate, and direction of change in binge drinking (e.g., escalation and desistance); and frequency of binge drinking.
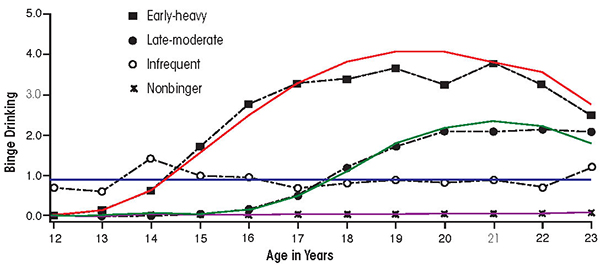
Most youth in community samples fall into the low-frequency binge-drinking and nonbinge-drinking trajectories. In some studies, nonbinge trajectories may include youth who drink but do not report binge episodes, as well as abstainers.59,60 Trajectories indicating persistence of binge drinking from adolescence into young adulthood, which typically represent a minority of youth in community samples, tend to show onset of binge drinking in early adolescence (i.e., at ages 12 to 13) and an increase to weekly or more frequent binges by late adolescence (i.e., at ages 17 to 18).7 Other binge-drinking trajectories are characterized by earlier (e.g., age 16 and younger) versus later (e.g., age 17 and older) onset of binge drinking or by a pattern of adolescent-limited binge drinking, in which binge drinking peaks in adolescence, then declines in early adulthood.7 One study that followed a high-risk sample of youth into young adulthood identified four types of binge-drinking† trajectories, including nonbinger (39.5%), infrequent (9.6%), late-onset moderate (30.0%), and early-onset heavy drinking (20.9%).57 Studies vary in the relative proportions of youth in each trajectory type because of methodological factors, such as differences in sampling (e.g., community vs. high-risk sample), age range, binge-drinking definition, and whether nonbinge trajectories include both abstainers and drinkers who do not report binge episodes.
†The study defined binge drinking as “5+ drinks in a row.”
Correlates of Adolescent Binge-Drinking Trajectories: Risk Factors and Young-Adult Outcomes
Distinct trajectories of binge drinking are thought to reflect different etiologic mechanisms.64 According to an ecological systems model,36,65 these etiologic mechanisms represent multiple systems (e.g., family, peer group, and community) that interact across development to influence binge-drinking trajectories.
Developmental factors associated with an increase in binge drinking during adolescence include, for example, reduced parental monitoring as youth mature37,66 and greater independence (e.g., obtaining a driver’s license) in daily activities.36 In addition, for some youth, onset of binge drinking may be associated with important school transitions (e.g., junior high to high school or high school to college), which can involve restructuring of peer groups and increased opportunities to engage in alcohol use.36 Importantly, processes of peer selection and peer influence have been associated with changes in binge drinking in adolescence.67-69 In particular, selection of peers who engage in binge drinking has been associated with an adolescent’s initiation and frequency of binge drinking.69
Several studies analyzed factors associated with binge trajectories, relative to nonbinge trajectories, at the individual level. Nonbinge trajectories in these studies included youth who abstained and youth who reported alcohol use below a given binge threshold. Risk factors identified in these studies included, for example, engaging in delinquent behavior, exposure to more stressful life events, and lower task persistence.61-63 Some of these risk factors may be associated with gender; for example, females may be more likely to experience certain stressful life events (e.g., sexual trauma), whereas males may be more likely to be involved in delinquent behavior or to show lower levels of impulse control.44,70 Moreover, in contrast to youth in binge-drinking trajectories, youth in nonbinge trajectories were more likely to report greater self-efficacy to resist social pressure to engage in substance use,62 as well as greater religiosity.63
With regard to the social context in which youth are nested, parental alcoholism and disrupted family relations (e.g., parental separation or divorce) each were associated with binge-drinking trajectories.57,62 Conversely, an adolescent’s perception of high pa-rental disapproval of substance use was prospectively associated with a nonbinge trajectory.60 Peer relations also had an impact, because changes in binge drinking tended to occur in parallel with changes in affiliation with drinking peers.60 However, despite the robust influence of peers on drinking behavior, an adolescent’s report of high parental disapproval of substance use weakened the effect of peers on binge drinking,60,69 indicating the important role that parents play in providing clear messages to their children regarding disapproval of underage drinking. It is important to note, however, that many individual and social risk factors associated with adolescent alcohol and other substance use have a more general influence and are not necessarily specific to binge drinking.
Community-level influences on adolescent binge-drinking trajectories include factors such as neighborhood and school environments, as well as local alcohol regulatory policies and enforcement. For example, one study found that youth living in neighborhoods with higher densities of on-premise alcohol outlets (e.g., bars and nightclubs) were more likely to report binge drinking, controlling for neighborhood-level socioeconomic status.71 However, neighborhood risks may be buffered by protective factors. In particular, a recent study found that a supportive school environment (e.g., alcohol prevention incorporated into the curriculum) was associated with reduced adolescent binge drinking over and above individual, family, and peer risk factors.72 Further, comprehensive and stringent local alcohol control policies and enforcement have been associated with lower levels of youth binge drinking, highlighting the importance of these community-level factors.73 The unique and cumulative effects of family, peer, and community influences on youth binge drinking emphasize the need for coordinated, developmentally tailored prevention programs that address each of these multiple interacting social systems to reduce risk.
Compared with nonbinge trajectories, binge-drinking trajectories in adolescence, particularly frequent and chronic binge drinking, have been associated with poorer functioning in young adulthood. For example, youth in binge trajectories were more likely to have an alcohol or other drug use disorder in young adulthood than those in nonbinge trajectories (which may include abstainers and youth who drink, but do not report binge episodes, depending on the study).57,62,74,75 In contrast, youth in nonbinge trajectories had better young-adult outcomes across domains such as educational attainment and employment, family and peer relations, and mental and physical health than did those in binge trajectories, particularly those who engaged in frequent, chronic binge drinking.57,59,62,76
Other analyses have compared different binge-drinking trajectories (e.g., chronic vs. adolescent-limited). Such studies found that compared with adolescent-limited trajectories, chronic binge-drinking trajectories exhibited stronger associations with other substance use75 and with stressful life events.63 Further, compared with alcohol use that did not meet definitions of binge drinking (i.e., less than five drinks per occasion), adolescent binge drinking (five or more drinks per occasion) was associated with adverse outcomes, such as lower academic performance, greater likelihood of reporting drunk driving in the past month, and other substance use.58 In sum, a pattern of relatively frequent and chronic binge drinking during adolescence, compared to nonbinge trajectories, was associated with worse young-adult outcomes across multiple domains, including risk for substance use disorder.
Neurocognitive Consequences of Adolescent Binge Drinking
In the context of the ongoing brain maturation that occurs in adolescence and young adulthood,77,78 binge drinking could result in potentially long-lasting neural alterations. For example, in rodent models, a binge pattern of alcohol exposure in adolescence has been associated with disrupted hippocampal functioning.79 Further, animal models indicate that binge alcohol exposure during adolescence can have downstream effects on cognition and behavior through epigenetic mechanisms.80,81 The specific effects of binge drinking during adolescence on the brain and neurocognition may depend on the timing, dose, and chronicity of alcohol exposure.38,82
Similar to animal research, in studies of human adolescents, heavy drinking has been associated with deficits in neuropsychological functioning83,84 and aberrations in brain structure and functioning.85-88 Some research suggests possible gender-specific ad-verse consequences of binge alcohol consumption on neurocognition.89 However, other research has found no difference between adolescent heavy drinkers (defined as 5+/6+ glasses, 10 g alcohol per glass, per occasion for females/males at least weekly) and light/nondrinkers in the maturation of basic executive functions (e.g., working memory).90 Overall, binge drinking in human adolescents may have relatively subtle effects on neuropsychological measures at the level of behavioral performance; given relatively short drinking histories among youth, differences between young binge drinkers and their healthy counterparts more readily are observed at the level of brain structure and functioning.86 Importantly, research suggests that after controlling for overall quantity of alcohol consumed, a binge pattern (i.e., consuming five or more drinks per occasion vs. consuming fewer than five drinks per occasion), in particular, was associated with adverse effects on brain functioning in young adults.91
Because most of the existing studies on binge drinking and neurocognition in human adolescents have been cross-sectional, the extent to which the findings reflect preexisting characteristics or persistent (vs. possibly transient) consequences of heavy or binge alcohol use are unclear. However, emerging research suggests that aberrations in the brain circuitry underlying decision-making may not only signal risk for binge drinking in adolescence prior to heavy drinking92 but also may be adversely affected by binge drinking in adolescence and young adulthood.93 The reversibility of the effects of adolescent binge drinking on brain structure and functioning with sustained abstinence warrants study, particularly because brain maturation continues into young adulthood.78 Large ongoing multisite studies, such as the National Consortium on Alcohol and Neurodevelopment in Adolescence,94 the IMAGEN study in Europe,95 and the Adolescent Brain and Cognitive Development Study (https://abcdstudy.org), which are examining the effects of alcohol and other substance use on the developing brain in adolescence, are poised to address these gaps in knowledge.
Implications for Prevention and Intervention
To reduce binge drinking, coordinated prevention and intervention efforts that operate across multiple levels (e.g., individual, family, community, and national policy), as well as continue across the life span, are needed.1,21 Such prevention efforts should be timed to begin by late childhood and should be tailored to address risks most salient to specific developmental periods and individual circumstances. For example, gender differences in risk factors for underage drinking44,70 suggest the potential utility of gender-specific interventions. Increasingly, developmental neuroscience provides the basis for novel prevention and intervention approaches that strengthen the social-emotional and decision-making skills needed to refrain from binge drinking, such as emotion regulation or resisting peer pressure to engage in risky behavior.95,96 Additional interventions for youth are needed that address alcohol’s strongly perceived positive effects. One approach may be to support alternative socially based rewarding and healthy activities, because experiencing adverse alcohol-related consequences may not reduce binge drinking in young populations.12
Ideally, prevention should include routine alcohol screening and brief intervention for all youth, as well as supportive guidance for parents and caregivers.97,98 Community-based prevention and intervention programs have shown effects in reducing underage drinking.99 School-based programs100 and easy access to a continuum of services4 are other examples of community-level supports for youth and families. At the level of public policy, strong alcohol policy environments101 and enhanced enforcement of local alcohol regulatory policies,102 such as the minimum legal drinking age and social-hosting laws, have deterred underage drinking.4
Conclusions
Adolescence is a critical period of risk for binge drinking. An adolescent-specific sensitivity to alcohol’s effects may interact with a normative propensity for greater risk-taking behavior and peer social environment in contributing to risk for binge drinking during this developmental period. Although there is debate regarding the definition of a binge-drinking episode, a dose-response relationship between episodic high-quantity alcohol consumption and increased risk for adverse consequences generally has been observed.18-20 Binge drinking in adolescence has been associated with multiple acute harms to health,4 including possible effects of heavy drinking on neuropsychological functioning83,84,87 and potential longer term adverse young-adult outcomes.57 Of particular concern is emerging research with young adults, which suggests that certain negative consequences of alcohol use on neurocognition may be specific to a binge pattern of alcohol consumption.91 Although the prevalence of adolescent binge drinking has declined since the 1970s, rates are still high. Moreover, binge-drinking prevalence likely is underestimated by surveys that use a binge definition of five or more drinks per occasion, because lower drinking-quantity thresholds to define binge drinking may be indicated, particularly for youth. Strategically coordinated prevention programs that operate across the life span and at multiple levels, ranging from individuals and families to public policy, are essential to reducing adolescent binge drinking.
Acknowledgments
This work was supported by NIAAA and other National Institutes of Health (NIH) grants: R01-DA-012237 (Dr. Chung), T32-AA-007453 (Dr. Bachrach), R01-AA-016482 and U01-AA-021690 (Dr. Clark), R01-AA-021721 and K24-AA-020840 (Dr. Martin), and L30-AA-022509 (Dr. Creswell).
Disclosures
The authors declare that they have no competing financial interests.