
Volume 39, Issue 1 ⦁ Pages: 31-42
Abstract
This article reviews literature aiming to explain the widespread reductions in binge and problem drinking that begin around the transition to young adulthood (i.e., “maturing out”). Whereas most existing literature on maturing out emphasizes contextual effects of transitions into adult roles and responsibilities, this article also reviews recent work demonstrating further effects of young adult personality maturation. As possible mechanisms of naturally occurring desistance, these processes could inform both public health and clinical interventions aimed at spurring similar types of drinking-related behavior change. This article also draws attention to evidence that the normative trend of age-related reductions in problem drinking extends well beyond young adulthood. Specific factors that may be particularly relevant to problem drinking desistance in these later periods are considered within a broader life span developmental framework.
Binge drinking is strikingly prevalent in the United States. An estimated 66.7 million (24.9%) of Americans age 12 or older report binge drinking in the past month, according to the National Survey on Drug Use and Health (NSDUH).1 This estimate is based on a binge drinking definition of 4 or more drinks on the same occasion for women, and 5 or more drinks on the same occasion for men, on at least 1 day in the past 30 days (see Drinking Patterns and Their Definitions in this issue for a review of binge drinking definitions). In addition to high binge drinking rates, alcohol use disorder (AUD) is among the most prevalent mental health disorders in the United States. An estimated 15.7 million (5.9%) of Americans age 12 or older have a past-year AUD diagnosis.1 These rates are a public health concern, as problem drinking in the United States costs an estimated $249 billion per year2 and is the fourth-leading cause of preventable mortality.3
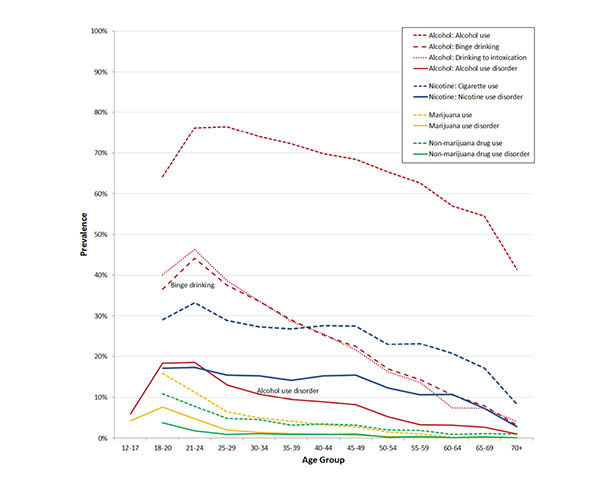
Perhaps the most striking demographic feature of problem drinking (and various other risky or deviant behaviors) is its nonlinear association with age, characterized by increases during adolescence, peaks around ages 18 to 22, and reductions beginning in the mid-20s.4 However, studies showing age differences in drinking-related rates for epidemiologic purposes tend to contrast relatively broad age groups, and a finer-grained depiction is informative from a developmental standpoint. Figure 1 shows the results of the authors’ descriptive analyses of age-prevalence gradients for different drinking-related outcomes (and other drug-related outcomes included for contrast).
As shown in Figure 1, prevalence rates for a variety of drinking-related outcomes peak in the early 20s. Specifically, in the early 20s, past-year binge drinking and intoxication rates both reach peaks of around 45%, and past-year AUD rates reach a peak of 19%. Although not depicted, similar drinking-related peaks are observed for college students and their noncollege peers, suggesting the peaks are at least partially driven by more general mechanisms beyond college attendance.5 Regarding historic trends, drinking-related declines have been observed across adolescent cohorts in recent years. For instance, 12th-grade rates of past 2-week binge drinking decreased from a peak of 32% in 1998 to an historic low of 17% in 2015.6 However, college students and young adults have had far more modest cohort declines in binge drinking (i.e., from a 39% peak in 2008 to 32% in 2015 for college students, and from a 41% peak in 1997 to 32% in 2015).6 Similar conclusions regarding historic changes across adolescent and young adult cohorts can be drawn from NSDUH data on AUD.1
Figure 1 also shows that, following peak prevalences in the early 20s, reliable age-related reductions in a variety of drinking-related outcomes occur beginning in the mid-20s and continue throughout the remainder of the life span. For instance, after the peak binge drinking rate of 45% in the early 20s, the rate declines to 38% by the late 20s, 29% by the late 30s, 22% by the late 40s, and 14% by the late 50s. For AUD, reductions appear especially dramatic in young adulthood. Specifically, after peaking at 19% in the early 20s, the rate decreases rapidly to 13% by the late 20s, then more gradually to 10% by the late 30s, 8% by the late 40s, and 3% by the late 50s. Of course, such cross-sectional age differences must be interpreted with caution, as differential mortality of problem drinkers and secular changes in prevalence rates could artifactually create the appearance of a developmental age gradient. However, it is unlikely that such factors could plausibly explain the magnitude of the rate changes with age, given the somewhat limited extent of overall mortality and secular variation. Further, researchers have also observed the age-prevalence curve in a number of longitudinal studies assessing how prevalence rates change as a cohort ages.7
This robust age-prevalence curve motivates and informs the conceptualization of problem drinking from a developmental psychopathology standpoint.8,9 Other articles in this special issue describe factors contributing to the escalation and eventual peak of problem drinking leading up to the early 20s. This article focuses on factors contributing to the later trends toward problem-drinking reductions beginning around young adulthood.
Maturing Out of Problem Drinking
The dramatic age-related reductions in problem drinking that begin in young adulthood have motivated empirical efforts to understand desistance from a developmental perspective. Despite the overall trend toward maturing out after young adulthood, a substantial subset of individuals show persistent or escalating problem drinking beyond this developmental period.10 Knowledge of what differentiates developmentally limited versus persistent patterns of problem drinking can help clarify the nature of problem drinking and inform public health and clinical interventions.11 Indeed, in addition to the above evidence that maturing out can include desistance of syndromal AUD, research also suggests that problem-drinking reductions during young adulthood are particularly likely to occur among those who were relatively severe problem drinkers prior to this developmental period.12,13 These findings support the importance of research aimed at understanding maturing out as a means of guiding future interventions.
The following sections review evidence for different possible mechanisms of maturing out, beginning with effects of adult role transitions (e.g., marriage and parenthood) and personality maturation (e.g., decreased impulsivity and neuroticism) during young adulthood. Further sections then discuss the need for more life span developmental research to explain the later drinking reductions observed in developmental periods beyond young adulthood, noting some mechanisms that may be particularly relevant to desistance in these periods (i.e., “natural recovery” processes and health issues). A key point pertaining to all mechanisms reviewed here is that more research is needed on possible historic changes in how these mechanisms have operated. Preliminary descriptive evidence suggests historic differences across cohorts in the age-related trend of escalation followed by maturing out.5(pp221-222) Key public policy insights could be gleaned from in-depth analyses of such cohort changes in age trends and how they may relate to cohort changes in desistance mechanisms (e.g., the prevalence, life-course timing, and impact of adult role transitions). It is also noteworthy that evidence exists for gender, racial, and ethnic differences in both patterns and mechanisms of age-related drinking reductions.4,7,14 Although discussion of such differences is largely beyond the scope of the current brief review, this should be noted as another important topic in need of further exploration in future research.
Young Adult Role Transitions and Maturing Out
The most commonly offered explanation for maturing out of problem drinking during young adulthood is that it is driven by transitions into adult roles like marriage, parenthood, and full-time employment.15 Young adulthood is marked by widespread adoption of such roles,15 and well-established developmental theory views these transitions as key young adult developmental tasks.16 Role incompatibility theory is often referenced to explain how these roles influence maturing out.17 The theory holds that, when a state of conflict (i.e., incompatibility) exists between a behavior (e.g., drinking) and demands of a social role, this can initiate a process called role socialization, whereby conflict is resolved through changes in the behavior. However, the theory also posits role selection effects in the opposite direction, whereby individual characteristics and behaviors can influence the likelihood of later role adoption. These are two very different processes through which roles and drinking behaviors can become associated, so research investigating possible role socialization effects must consider role selection as an alternative explanation.
Evidence for Role Socialization
With few exceptions,18-20 both marriage and parenthood during young adulthood are generally predictive of later problem-drinking reductions. Further, although many studies have tested only effects of either marriage or parenthood in isolation,21-28 there is also research demonstrating that both marriage and parenthood can contribute uniquely to these reductions.15,29,30 In contrast, research has often failed to show that employment contributes to reduced problem drinking in young adulthood,15,24,27 although some evidence for this effect has been found within certain occupational categories (e.g., “professional” jobs).30
Evidence for Role Selection
Most studies have failed to show that alcohol use reduces the likelihood of young adult marriage, parenthood, or employment,21,27 with some findings even suggesting the opposite effect.15 However, results appear more mixed for more severe indices of problem drinking and for illicit substance use. For example, research has shown that AUD can prevent marriage and parenthood,31,32 and that illicit substance use can prevent marriage and employment.15,33-35
Practical Implications of Role Effects on Maturing Out
In addition to evidence that family roles can spur desistance from AUD,24,36 there is even evidence that these roles may have especially dramatic effects among those who were particularly severe problem drinkers prior to role adoption.37 These findings support the clinical significance, not only of maturing out in general, but of role-driven pathways to maturing out in particular. Further, beyond family role effects on drinking-related maturing out, there is mounting evidence from diverse literatures that family roles convey various protective effects that can cascade across many domains of life to broadly spur adaptation and mitigate pathology.38-41
However, given the potential importance of these processes from a public health standpoint, it is surprising how little is known about the mechanisms through which roles influence substance-related maturing out. Existing mediational findings show the most robust support for mediation of role effects via reduced socializing with peers, with additional mixed evidence for mediation via changes in drinking-related attitudes and increased religiosity.27,28,30,42 Mediation via peer involvement is particularly consistent with the popular role incompatibility explanation of family role effects on maturing out (described above), as role demands may restrict socializing opportunities. However, as articulated in Platt’s commentary on how to achieve “strong inference,” future studies should conduct “riskier” tests of role incompatibility theory.43 This means testing hypotheses that could potentially provide discriminating support for role incompatibility theory over other plausible explanations, and testing hypotheses that could potentially disconfirm the theory in favor of other explanations. For instance, an explicit assessment of conflict between drinking and role demands (role incompatibility) could provide discriminating support for role incompatibility theory,37 and this should be tested against other plausible mechanisms, such as the interpersonal support, security, and satisfaction that family roles can provide.44
Young Adult Personality Development and Maturing Out
A vast, long-standing literature links personality and drinking, although variability in personality models, definitions, and terminology can sometimes complicate interpretation of this work.45 For instance, “Big Three” models of the traits that compose personality typically include constraint (related to impulsivity and risk taking), neuroticism (e.g., anxiety, depression, and stress reactivity), and extraversion (e.g., sociability),46 whereas “Big Five” models typically include neuroticism, extraversion, conscientiousness, agreeableness, and openness (or intellect).47,48 Within Big Five models, distinct components of impulsivity and constraint (e.g., lack of perseverance and negative affect urgency) are represented as smaller facets of the larger broad- band traits (e.g., conscientiousness and neuroticism).49 It is beyond this brief review’s scope to broadly review the many ways these and other models of personality have been linked to drinking, but see Sher and colleagues for an in-depth review of personality and alcohol research.45
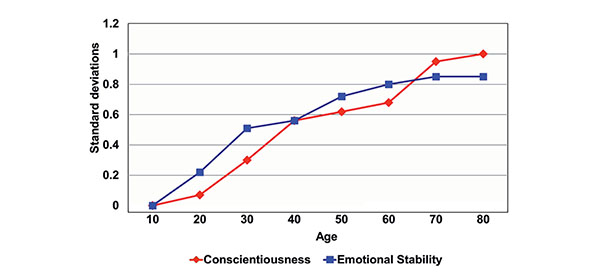
This review focuses on one particularly relevant burgeoning area of personality research that has emphasized movement beyond a static view of personality, acknowledging that normative changes in personality occur throughout the life span. Importantly, findings include evidence for adaptive (i.e., presumably beneficial) changes in personality traits that have been linked closely to heavy and problematic drinking, including impulsivity, conscientiousness, and neuroticism. Further, maturational changes in these traits appear particularly rapid during the transition to young adulthood (i.e., the 20s and 30s), the period when normative age-related declines in drinking generally begin. For instance, Figure 2 depicts meta-analytic evidence for age-related increases throughout the adult life span in both emotional stability (akin to lack of neuroticism) and conscientiousness.39,50,51
Correlated Change in Personality and Problem Drinking
Perhaps motivated by the above evidence for personality maturation, a subsequent series of studies has shown that the normative age-related drinking reductions of young adulthood may be partially explained by age-related personality change.52,53 Longitudinal growth models showed a reduction in average levels of problem drinking from ages 18 to 35, along with corresponding reductions in impulsivity and neuroticism and increases in conscientiousness. Further, parallel-process growth models showed correlated change such that those with greater age-related maturation in these three personality domains also had greater age-related reductions in problem drinking. A follow-up study using the same data also showed that age-related changes in drinking motives mediated effects of age-related personality change on age-related problem-drinking reductions.54 Specifically, reductions in neuroticism and impulsivity predicted reductions in coping-related drinking motives, which in turn predicted reductions in problem drinking. These are the only studies, to our knowledge, analyzing correlated change in personality and drinking as an explanation for the normative drinking reductions observed around the developmental transition to young adulthood (i.e., maturing out), although other studies have shown similar correlated change in earlier developmental periods of normative drinking-related escalation (i.e., adolescence to the early 20s).55
Directional Effects of Personality on Drinking Over the Course of Young Adulthood
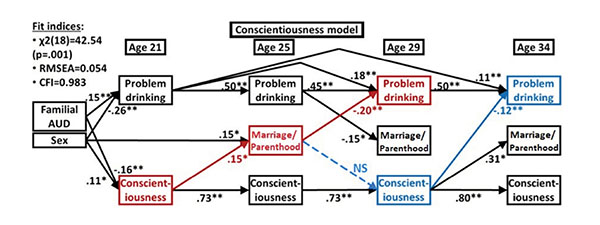
The above studies of correlated change between personality and problem drinking have forged an entirely new avenue for research on drinking-related maturing out, with one important next step being investigation of different possible directions of effects. Toward this objective, Lee and colleagues estimated cross-lag models testing bidirectional effects between personality and problem drinking across four waves spanning ages 21 to 34.56 Results showed some prospective effects of personality on problem drinking, with lower impulsivity and higher conscientiousness at age 29 both predicting lower problem drinking at age 34 (see Figure 3). In contrast, results did not show prospective effects of neuroticism on subsequent problem drinking (nor prospective effects in the opposite direction).
Integrating Adult Role and Personality Effects on Maturing Out
Beyond the largely separate bodies of evidence for family role and personality maturation effects on young adult drinking reductions, little work exists advancing an integrated model of these ameliorative processes. Differing views conceptualize personality maturation as unfolding either (1) due to biologically programmed maturation or (2) as an adaptive response to age-increasing contextual demands (e.g., from family roles).39 These alternative views imply different predictions regarding possible mediated pathways involving role and personality effects on problem-drinking reductions. To investigate these possibilities, the cross-lag models of Lee and colleagues (discussed above) also included transitions into family roles (marriage or parenthood).56 Results showed that family role transitions mediated personality effects, with higher conscientiousness and lower impulsivity at age 21 predicting transitions into a family role by age 25, which in turn predicted lower problem drinking at age 29 (see Figure 3). In contrast, personality was not found to mediate role effects, as role transitions consistently failed to predict later personality.
Practical Implications of Personality Development Effects on Maturing Out
The notion of interventions targeting personality change has received increased attention in recent literature.57 The above-discussed research on personality and maturing out has especially highlighted the potential utility of reducing impulsivity and increasing conscientiousness. Littlefield and colleagues speculated that interventions fostering maturity in these domains might spur relatively durable changes in drinking behaviors.52 Lee and colleagues noted, based on the above mediation findings, that pre–young adult personality interventions could convey protective effects, in part by aiding successful transitions to family roles in young adulthood.56 Based on evidence for persistent effects of childhood impulsivity even on midlife outcomes, Moffitt and colleagues argued that universal prevention programs fostering childhood self-control could confer substantial and lasting benefits to most individuals and to an entire population.58 Indeed, early prevention and intervention programs fostering personality-related maturity could influence many etiologic pathways, thereby conveying protective effects that cascade across multiple developmental stages and domains of life.
However, to bolster confidence in the above implications, additional research is needed to confirm and further characterize the phenomenon of personality maturation and its effects on age-related drinking reductions. Caution is perhaps warranted regarding the use of survey measures to show personality change, as measurement invariance across ages can spuriously influence apparent age-related changes.59 However, given the magnitude of personality change observed across the life span,39(p15) and its associations with changes in various life circumstances,50 it is unlikely that this phenomenon is largely attributable to a measurement artifact. Nonetheless, confidence could be bolstered by showing this phenomenon with alternative methods. For instance, given the existence of various task-based measures of impulsivity/disinhibition,60 a key objective should be to confirm age-related changes in these measures and their associations with age-related drinking reductions. Such research could confirm conclusions from survey findings and further inform the practical application of this work.
Further, although clear links have been established among personality maturation, adult role adoption, and drinking reductions, more work is needed to establish directionality of effects within analyses that unambiguously capture developmental change in these constructs. For instance, the cross-lagged panel study by Lee and colleagues56 addressed the unknown directionality in the growth-modeling studies of Littlefield and colleagues,52-54 but personality effects in the analyses by Lee and colleagues did not isolate influences of age-related change in personality traits. Thus, creative analytic applications are needed to combine the separate strengths of past research. This work also may require careful conceptualization of the predicted timings and durations of the developmental processes under investigation.
Maturing Out of Problem Drinking Beyond Young Adulthood
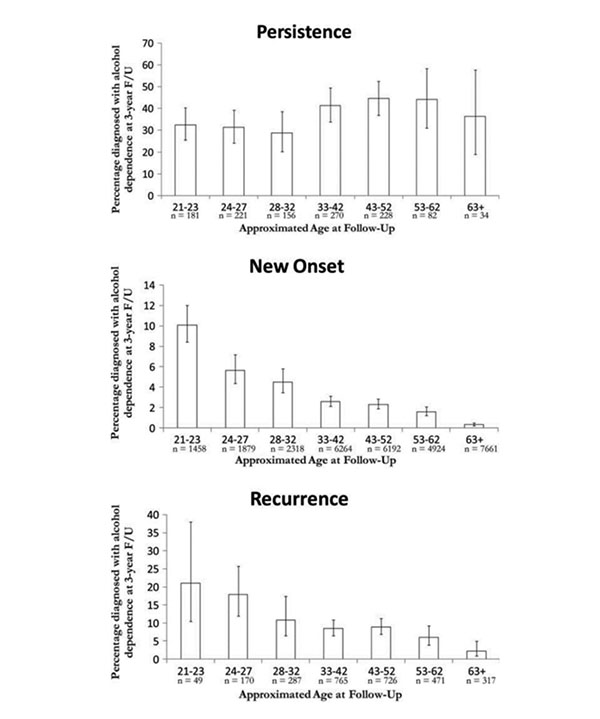
As discussed above, age-related drinking reductions are not confined to young adulthood, but instead begin in young adulthood and continue throughout the remaining life span. Beyond the earlier-reviewed epidemiologic evidence, some additional research offers a more precise account of changes in problem drinking across the adult life span. Vergés and colleagues assessed changes across the life span in rates of persistence, new onset, and recurrence of alcohol dependence to understand their unique contributions to overall age-related reductions in alcohol dependence rates.20 Results showed especially marked age reductions in new onsets (see Figure 4, middle panel). Thus, although the term “maturing out” may be taken to imply age increases in desistance, the continual declines in AUD rates observed throughout the life span instead appear mainly attributable to reductions in new onsets. In contrast, although not emphasized by Vergés and colleagues, rates of desistance appeared to peak in young adulthood. Based on persistence rates in their study, it can be inferred that the rate of desistance peaked at 72% by ages 28 to 32, then declined to a low of 55% by ages 43 to 52 and remained somewhat low thereafter (see Figure 4, upper panel). Thus, an interesting possibility is that risk for AUD onset may continually decline throughout the life span, whereas potential for desistance from an existing AUD may peak in young adulthood. Perhaps confirming and extending the latter notion, ongoing data analyses by the authors62 have investigated desistance across the life span while differentiating among mild, moderate, and severe AUD (per the Diagnostic and Statistical Manual of Mental Disorders [DSM-5] severity grading).63 Results showed that for those with a severe AUD, desistance rates were substantially higher in young adulthood than in later developmental periods (e.g., severe AUD desistance rates of 46% to 49% at ages 25 to 34 versus 25% to 29% at ages 35 to 55). Of course, given that both above studies used data from the U.S. National Epidemiologic Survey on Alcohol and Related Conditions (NESARC), these analyses should be replicated in other data sets.
The above evidence for differences across the life span in patterns of desistance suggests there may also be important differences across the life span in mechanisms of desistance. Assessing this possibility should be a key goal of future research, as researchers have clearly gleaned insights through similar attention to developmental variability in etiologic processes of earlier developmental periods (i.e., childhood and adolescence).64 The following sections consider some specific ways that the mechanisms influencing problem drinking desistance may vary across periods of the adult life span.
Maturing Out Versus Natural Recovery Models of Desistance
Predictions regarding developmental variability in desistance mechanisms can perhaps be made based on Watson and Sher’s review highlighting dramatic differences in how desistance is viewed between the “maturing out” and “natural recovery” literatures.65 As discussed earlier, the maturing out literature focuses on young adulthood and has largely viewed desistance as stemming from contextual changes in this developmental period (e.g., marriage)15 and accompanying role demands that conflict with alcohol involvement.17 Importantly, these processes are rarely conceptualized as involving acknowledgment or concern regarding one’s drinking.4,65 A starkly different view of desistance comes from the natural recovery literature, which has investigated precursors of desistance mostly in midlife samples (e.g., mean age = 41 years [SD = 9.1] in a review by Sobell and colleagues).66 Informed in part by models of behavior change (e.g., Stall and Biernacki’s stages of spontaneous remission),67 this literature often views desistance as stemming from an accumulation of drinking consequences that can prompt (1) deliberate reappraisals of one’s drinking, followed by (2) self-identification as a problem drinker (i.e., problem recognition), and then (3) targeted efforts to change drinking habits.68
Predictions can perhaps stem from an overarching premise that the maturing out and natural recovery literatures may both offer valid conceptualizations of desistance, with maturing out models applying predominantly to young adulthood and natural recovery models applying predominantly to midlife and later developmental periods. That is, desistance in young adulthood may more often stem from the broad cascade of maturational contextual changes that occurs in this period, whereas desistance in later periods may more often stem from more direct processes of deliberate problem recognition and change efforts.
These predictions are consistent with the general idea that contextual effects are stronger earlier in development, whereas intrapersonal effects increase with age69 as individuals increasingly construct their own environments.70 It is also noteworthy that there is conceptual similarity between the deliberate reappraisal of one’s drinking described in the natural recovery literature and the drinking attitude change believed to mediate personality maturation effects on drinking-related desistance, suggesting a possible point of overlap between natural recovery and personality maturation research. Thus, personality maturation in young adulthood (e.g., conscientiousness increases) may distally potentiate later natural recovery processes of problem recognition and effortful change. Although quite speculative, if the above predictions are supported, this would help bridge divides among different highly influential, yet ostensibly discrepant, views of desistance. More generally, investigating these predictions could help advance the field toward a more unified understanding of desistance across the life span and thereby inform developmental tailoring of public health and clinical interventions.
Older Adult Health and Problem Drinking Desistance
Although health and drinking are, of course, interrelated throughout the life span,71,72 older adulthood brings various health-related physical and cognitive challenges that may increase in importance as desistance mechanisms in this late developmental stage.73 There is evidence that more than 50% of U.S. seniors drink at levels deemed risky in the context of co-occurring medical conditions.74 Further, along with these health issues comes increased use of medications that could interact harmfully with alcohol, with a striking 76% of U.S. seniors using multiple prescription medications.75 Of the small extant literature on older adult drinking, health issues are among the most commonly reported reasons for desistance.76 However, studies of prospective effects of health problems on drinking changes are more equivocal,76,77 perhaps owing to the complex relevance of affect- and coping-related issues to older adult drinking.78 For instance, there is evidence that health problems can spur drinking reductions except among those who drink to cope, for whom health problems can have the opposite effect.77,79
Future studies should expand upon the relative dearth of research in this area. This work should include further study of how affect- and coping-related factors may impede adaptive responding to drinking-related health issues. Attention should also be paid to how these processes are influenced by aging-related increases in alcohol sensitivity80,81 and changes in social support systems.73 These questions are particularly important given the increases in older adult problem drinking that are projected to coincide with the aging of the “baby boomer” generation.82 Indeed, these projections suggest a great future need for research informing policy and clinical interventions for older adult problem drinkers.
Summary of Key Points
Although a distinct peak in problem drinking rates is observed in the early 20s, the reductions that follow (i.e., maturing out) are not confined to the subsequent period of young adulthood. Problem-drinking reductions continue throughout all remaining stages of the adult life span.
In addition to robust evidence that young adult desistance is spurred by transitions into family roles, more recent work shows additional likely influences of developmental personality maturation. Research is needed to further clarify these ameliorative influences, the mechanisms through which they operate, and how they are inter- related. Such work may yield key practical insights that could inform the design of clinical and public health interventions.
In contrast with developmental models of maturing out, other influential views of desistance (i.e., natural recovery models) place more emphasis on processes of problem recognition and effortful change. A life span developmental perspective on desistance may hold promise for reconciling these ostensibly discrepant models.
More research is needed on health-related mechanisms of problem drinking desistance among older adults.
Acknowledgments
Writing of this review was supported by National Institute on Alcohol Abuse and Alcoholism grant K99-AA-024236 to Dr. Lee and grants T32-AA-013526 and K05-AA-017242 to Dr. Sher.
Disclosures
The authors declare that they have no competing financial interests.